Taekwondo 태권도Taekwondo Preschool
Promotion from one geup to the next can proceed rapidly in some schools, since schools often allow geup promotions every two, three, or four months. Students of geup rank learn the most basic techniques first, and then move on to more advanced techniques as they approach first dan. Many of the older and more traditional schools often take longer to allow students to test for higher ranks than newer, more contemporary schools, as they may not have the required testing intervals. View Taekwondo belt levels »
About Achilles Tendon Rupture
Sports injuries are injuries that occur in athletic activities. They can result from acute trauma, or from overuse of a particular body part. Please see a certified specialist or doctor for sports injuries. Proper guidance and instructions are needed from a certified Master Instructor ( 사범님 sabeomnim ) to ensure safe training.
The Achilles tendon is the most commonly injured tendon. Rupture can occur while performing actions requiring explosive acceleration, such as pushing off or jumping. The male to female ratio for Achilles tendon rupture varies between 7:1 and 4:1 across various studies.

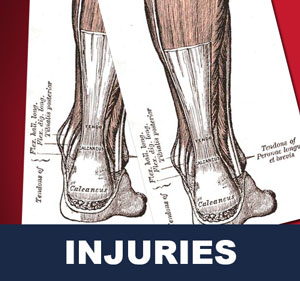
Anatomy
The Achilles tendon is the strongest and thickest tendon in the body, connecting the gastrocnemius, soleus and plantaris to the calcaneus. It is approximately 15 centimeters (5.9 inches) long and begins near the middle portion of the calf. Contraction of the gastrosoleus plantar flexes the foot, enabling such activities as walking, jumping, and running. The Achilles tendon receives its blood supply from its musculotendinous junction with the triceps surae and its innervation from the sural nerve and to a lesser degree from the tibial nerve.
Causes
The Achilles tendon is most commonly injured by sudden plantarflexion or dorsiflexion of the ankle, or by forced dorsiflexion of the ankle outside its normal range of motion.
Other mechanisms by which the Achilles can be torn involve sudden direct trauma to the tendon, or sudden activation of the Achilles after atrophy from prolonged periods of inactivity. Some other common tears can occur from overuse while participating in intense sports. Twisting or jerking motions can also contribute to injury.
Fluoroquinolone antibiotics, famously ciprofloxacin, are known to increase the risk of tendon rupture, particularly achilles.
Risk Factors
People who commonly fall victim to Achilles rupture or tear include recreational athletes, people of old age, individuals with previous Achilles tendon tears or ruptures, previous tendon injections or quinolone use, extreme changes in training intensity or activity level, and participation in a new activity.
Most cases of Achilles tendon rupture are traumatic sports injuries. The average age of patients is 29–40 years with a male-to-female ratio of nearly 20:1. Fluoroquinolone antibiotics, such as ciprofloxacin, and glucocorticoids have been linked with an increased risk of Achilles tendon rupture. Direct steroid injections into the tendon have also been linked to rupture.
Quinolone has been associated with Achilles tendinitis and Achilles tendon ruptures for quite some time now. Quinolones are antibacterial agents that act at the level of DNA by inhibiting DNA Gyrase. DNA Gyrase is an enzyme used to unwind double stranded DNA which is essential to DNA Replication. Quinolone is specialized in the fact that it can attack bacterial DNA and prevent them from replicating by this process, and are frequently prescribed to elderly. Approximately 2% to 6% of all elderly people over the age of 60 that have had Achilles ruptures can be attributed to the use of quinolones.
Diagnosis
Diagnosis is made by clinical history; typically people say it feels like being kicked or shot behind the ankle. Upon examination a gap may be felt just above the heel unless swelling has filled the gap and the Simmonds' test (aka Thompson test) will be positive; squeezing the calf muscles of the affected side while the patient lies prone, face down, with his feet hanging loose results in no movement (no passive plantarflexion) of the foot, while movement is expected with an intact Achilles tendon and should be observable upon manipulation of the uninvolved calf. Walking will usually be severely impaired, as the patient will be unable to step off the ground using the injured leg. The patient will also be unable to stand up on the toes of that leg, and pointing the foot downward (plantarflexion) will be impaired. Pain may be severe, and swelling is common.
An O'Brien test can also be performed which entails placing a sterile needle through the skin and into the tendon. If the needle hub moves in the opposite direction of the tendon and the same direction as the toes when the foot is moved up and down then the tendon is at least partially intact.
Sometimes an ultrasound scan may be required to clarify or confirm the diagnosis. MRI can also be used to confirm the diagnosis.
Treatment
Treatment options for an Achilles tendon rupture include surgical and non-surgical approaches. Among the medical profession opinions are divided what is to be preferred.
Non-surgical management traditionally was selected for minor ruptures, less active patients, and those with medical conditions that prevent them from undergoing surgery. It traditionally consisted of restriction in a plaster cast for six to eight weeks with the foot pointed downwards (to oppose the ends of the ruptured tendon). But recent studies have produced superior results with much more rapid rehabilitation in fixed or hinged boots.
Some surgeons feel an early surgical repair of the tendon is beneficial. The surgical option was long thought to offer a significantly smaller risk of re-rupture compared to traditional non-operative management (5% vs 15%). Of course, surgery imposes higher relative risks of perioperative mortality and morbidity e.g. infection including MRSA, bleeding, deep vein thrombosis, lingering anesthesia effects, etc.
However, four recent studies have scientifically tested the benefits of surgery, using randomized streaming of patients into surgical and non-surgical protocols, and applying virtually identical (and aggressive) rehabilitation protocols to both types of patients. All four such studies completed to date have found only small, but statistically significant benefits from the surgery, separated from the other confounding variables. They have all produced reasonably comparable results in re-rupture rates (with each study adding a cautious note about small sample size, one study showing 12% re-rupture in non-surgical treatment versus 4% re-rupture in surgical treatment, which is statistically insignificant), strength, and range of motion, while most have reaffirmed the greater complication rate from surgery. Two studies showed small, but statistically significant differences in plantarflexion strength. The surgical group had significantly better results in the heel-rise work, heel-rise height, concentric power, and hopping tests at the 6-month evaluation than did the nonsurgical group. However, at the 12-month evaluation, there was a significant between-groups difference only in the heel-rise work test.
The relative benefits of surgical and nonsurgical treatments remains a subject of debate; authors of studies are cautious about the preferred treatment. It should be noted that in centers that do not have early range of motion rehabilitation available, surgical repair is preferred to decrease re-rupture rates.
Rehabilitation
Non-surgical treatment used to involve very long periods in a series of casts, and took longer to complete than surgical treatment. But both surgical and non-surgical rehabilitation protocols have recently become quicker, shorter, more aggressive, and more successful. It used to be that patients who underwent surgery would wear a cast for approximately 4 to 8 weeks after surgery and were only allowed to gently move the ankle once out of the cast. Recent studies have shown that patients have quicker and more successful recoveries when they are allowed to move and lightly stretch their ankle immediately after surgery. To keep their ankle safe these patients use a removable boot while walking and doing daily activities. Modern studies including non-surgical patients generally limit non-weight-bearing (NWB) to two weeks, and use modern removable boots, either fixed or hinged, rather than casts. Physiotherapy is often begun as early as two weeks following the start of either kind of treatment.
There are three things that need to be kept in mind while rehabilitating a ruptured Achilles: range of motion, functional strength, and sometimes orthotic support. Range of motion is important because it takes into mind the tightness of the repaired tendon. When beginning rehab a patient should perform stretches lightly and increase the intensity as time and pain permits. Putting linear stress on the tendon is important because it stimulates connective tissue repair, which can be achieved while performing the “runners stretch,” (putting your toes a couple inches up the wall while your heel is on the ground). Doing stretches to gain functional strength are also important because it improves healing in the tendon, which will in turn lead to a quicker return to activities. These stretches should be more intense and should involve some sort of weight bearing, which helps reorient and strengthen the collagen fibers in the injured ankle. A popular stretch used for this phase of rehabilitation is the toe raise on an elevated surface. The patient is to push up onto the toes and lower his or her self as far down as possible and repeat several times. The other part of the rehab process is orthotic support. This doesn’t have anything to do with stretching or strengthening the tendon, rather it is in place to keep the patient comfortable. These are custom made inserts that fit into the patients shoe and help with proper pronation of the foot, which is otherwise a problem that can lead to problems with the Achilles.
To briefly summarize the steps of rehabilitating a ruptured Achilles tendon, you should begin with range of motion type stretching. This will allow the ankle to get used to moving again and get ready for weight bearing activities. Then there is functional strength, this is where weight bearing should begin in order to start strengthening the tendon and getting it ready to perform daily activities and eventually in athletic situations.
















Related Articles
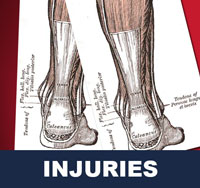
Sports injuries are injuries that occur in athletic activities such as in taekwondo. They can result from acute trauma, or from overuse of a particular body part. Collisions with the ground, objects, and other practitioners are common, and unexpected dynamic forces on limbs and joints can cause injury. View Sport Injuries »
- Achilles Tendon - the Achilles tendon is the most commonly injured tendon. Rupture can occur while performing actions requiring explosive acceleration, such as pushing off or jumping.
- Bone Fracture - a bone fracture is a medical condition in which there is a break in the continuity of the bone. A bone fracture can be the result of high force impact or stress, or a minimal trauma injury as a result of certain medical conditions that weaken the bones, such as osteoporosis, bone cancer, or osteogenesis imperfecta.
- Pulled Hamstring - defined as an excessive stretch or tear of muscle fibers and related tissues. Hamstring injuries are common in athletes participating in many sports and are very difficult to treat and rehabilitate.
- Sprain - damage to one or more ligaments in a joint, often caused by trauma or the joint being taken beyond its functional range of motion. The severity of sprain ranges from a minor injury which resolves in a few days to a major rupture of one or more ligaments requiring surgical fixation and a period of immobilisation.
- Sprained Ankle - also known as an ankle sprain, twisted ankle, rolled ankle, floppy ankle, ankle injury or ankle ligament injury, is a common medical condition where one or more of the ligaments of the ankle is torn or partially torn.
- Strain - an injury to a muscle in which the muscle fibers tear as a result of overstretching. A strain is also colloquially known as a pulled muscle. The equivalent injury to a ligament is a sprain.
Taekwondo Basics
Here is where you can learn more about Taekwondo 태권도. Knowing the fundamental basics is very important for your learning path as you build your skills and knowledge. There are certain rules that need to be followed to show respect to the master ( 사범님 sabeomnim ), the instructors ( 교사님 gyosannim ), other practitioners and to the martial arts. They vary between schools but many have similar rules and guidelines. For more information View Taekwondo Basics »
Please see a certified specialist or doctor for sports injuries. The article provided on this page is information that is widely available on Wikipedia article "Achilles Tendon Rupture". Risk of injury can be reduced by completing an effective warm up consisting of a heart raiser to get your pulse up, followed by sport specific dynamic stretches (stretches whilst moving). Please follow the guidance of a certified Master Instructor or trainer when doing sports related activities.
RESOURCES
This article uses material from the Wikipedia article "Achilles Tendon Rupture", which is released under the Creative Commons Attribution-Share-Alike License 3.0.


")
")


